1)Hu T, et al. : Prevalence of depression in older adults: A systematic review and meta-analysis. Psychiatry Res, 311 : 114511, 2022.
2)日本うつ病治療ガイドライン. 高齢者のうつ病治療ガイドライン. 日本うつ病学会, 2020.
3)David M., et al. : The Maudsley Prescribing Guidelines in Psychiatry, 14th edition. 2021.
4)Tham A, et al. : Efficacy and tolerability of antidepressants in people aged 65 years or older with major depressive disorder – A systematic review and a meta-analysis. J Affect Disord, 205 : 1-12, 2016.
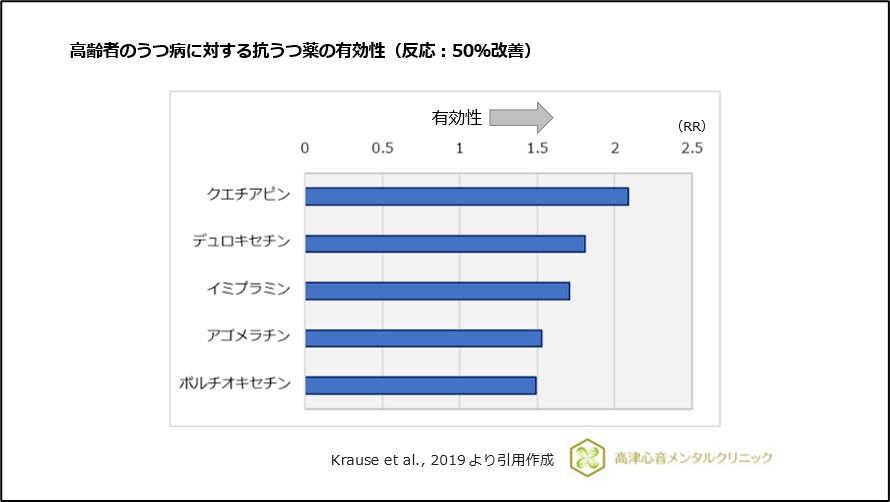
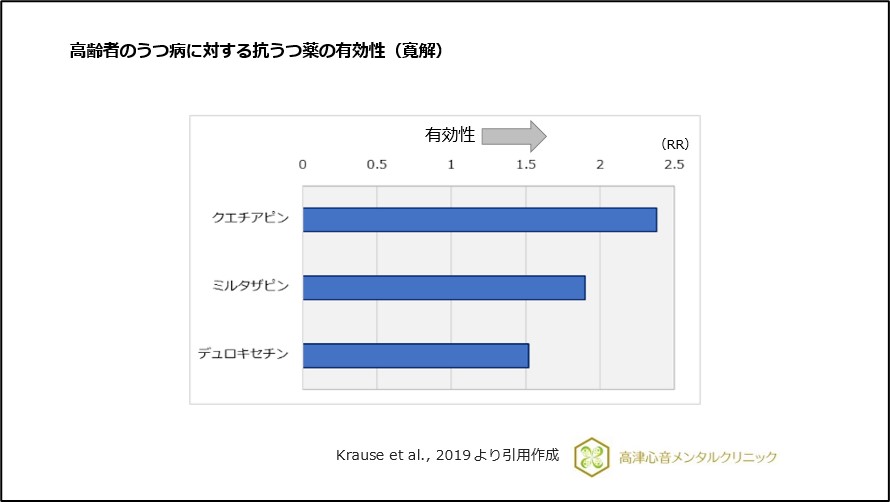
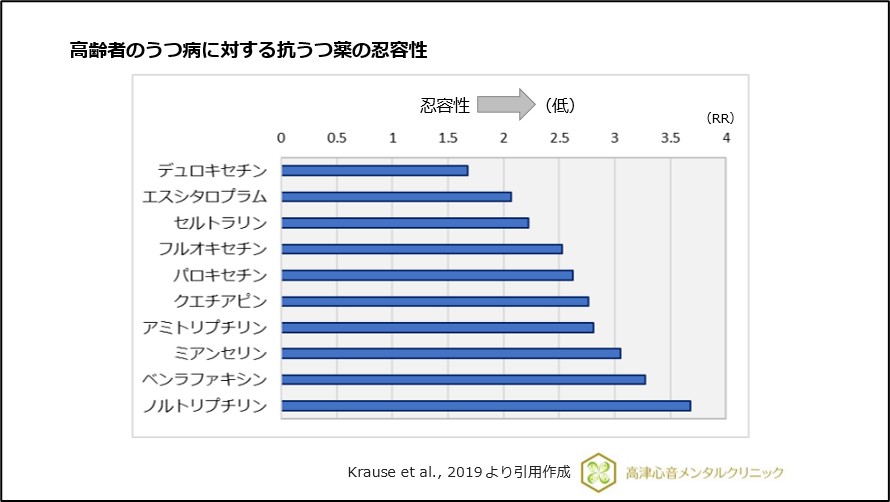
5)Krause M, et al. : Efficacy and tolerability of pharmacological and non-pharmacological interventions in older patients with major depressive disorder: A systematic review, pairwise and network meta-analysis. Eur Neuropsychopharmacol, 29 : 1003-1022, 2019.
6)Dhillon S.: Duloxetine: a review of its use in the management of major depressive disorder in older adults. Drugs Aging, 30 : 59-79, 2013.
7)Sobieraj DM, et al. : Adverse Effects of Pharmacologic Treatments of Major Depression in Older Adults. J Am Geriatr Soc, 67 : 1571-1581, 2019.
8)Maier A, et al. : Risk factors and protective factors of depression in older people 65+. A systematic review. PLoS One, 16 : e0251326, 2021.
9)Lin Y, et al. : Effectiveness of horticultural therapy on physical functioning and psychological health outcomes for older adults: A systematic review and meta-analysis. J Clin Nurs, 31 : 2087-2099, 2022.
10)Zhang YW, et al. : The effect of horticultural therapy on depressive symptoms among the elderly: A systematic review and meta-analysis. Front Public Health, 10 : 953363, 2022.
11)Domènech-Abella J, et al. : Anxiety, depression, loneliness and social network in the elderly: Longitudinal associations from The Irish Longitudinal Study on Ageing (TILDA). J Affect Disord, 246 : 82-88, 2019.
12)Santini ZI, et al. : Social disconnectedness, perceived isolation, and symptoms of depression and anxiety among older Americans (NSHAP): a longitudinal mediation analysis. Lancet Public Health, 5 : e62-e70, 2020.